
The rapid spread of the Omicron variant has led to a dramatic increase in the number of people under the age of 18 going to hospital in the United States.
Now, a University of Toronto health researcher says that based on U.S. data, it’s reasonable to suggest that the Omicron variant could result in about 800 B.C. children and youths being admitted to hospital with COVID-19 within a month.
Colin Furness, an assistant professor in the Dalla Lana School of Public Health, drew this conclusion during a January 6 online discussion hosted by Protect Our Province B.C., which is a group of health-care workers and researchers.
It came in response to a question by the moderator, Dr. Brenda Hardie, about whether Omicron is mild.
Furness admitted that his estimate was based on some back-of-the-envelope math.
He divided the U.S. population by the number of U.S. residents under the age of 18 who had been admitted to hospital because of COVID-19.
Then he did the same arithmetic by substituting the B.C. population. That resulted in 78 admissions to hospital per week of people under the age of 18 due to COVID-19.
Next, he incorporated the U.S. growth rate in admissions—a 65 percent hike in the last week of December over the previous week.
“This rate of increase may continue,” Furness said. “It may pick up speed. It may level off. The fact of the matter is truly, we don’t know.”
While he acknowledged that this is a “very simplified projection”, he said that it should also be alarming. That’s because 800 child admissions to hospital in B.C. within one month would create a strain on the health-care system.
That’s especially so, given risk factors for serious COVID-19 within some elements of the child and youth population.
For example, he said that infants under three months are 7.8 times as likely to develop serious symptoms requiring hospitalization.
“Now, we can’t stop people being under three months of age and we can’t isolate them from their parents and their siblings and the community,” Furness said. “We can’t Saran-wrap them. We can’t. So they are enormously at risk.”
Those children and youths with diabetes are 6.6 times more likely to have serious COVID, he added.
He noted that those born prematurely have a 3.7 times greater chance of suffering serious symptoms because early birth has immune-system implications.
The risk is slightly lower for those with compromised immunity.
Moreover, he said that kids with asthma have more than double the chance of suffering serious COVID.
Furness also expressed alarm over B.C.’s very small number of pediatric intensive-care-unit beds.
There are only 28 pediatric intensive-care unit beds to “provide the highest quality of care to critically ill children” in B.C. Children’s Hospital, according to the hospital website.
Read a transcript of Furness’s remarks
Dr. Brenda Hardie: Is Omicron mild?
Colin Furness: That is a vital question and it’s actually an incredibly complicated question packed into so few words.
The first part of the answer is it depends on whether you frame COVID as a respiratory virus. If you frame it as a respiratory virus, you have permission to call it mild, to say it’s nothing but sniffles for kids. And that’s commonly out there and I’ve heard that articulated in B.C. and elsewhere.
But here’s the thing: COVID, before we even get to Omicron, COVID is not a respiratory disease. It’s a vascular disease that has an initial respiratory phase in kids and increasingly in adults. The respiratory phase is less dangerous, less acute. It looks like sniffles.
The problem is not the sniffles. The problem is what the virus is doing elsewhere in the body from the toes to the testes to the brain. It is causing autoimmune disease. It is causing loss of brain tissue.
We haven’t seen that in children because we haven’t looked. But we have seen it in adults, literally—brain tissue disappearing. And autopsies of bodies have shown residual virus present six months after infection. Six months.
So this virus only begins in the lungs. And if all we’re going to talk about is lungs—and I really, really dislike that framing—then we can call it mild but I’m unprepared to do that.
And you know, I find that infectious-disease doctors are not speaking up about this. This is their wheelhouse. I don’t want to pretend to be an infectious-disease physician. I don’t want to pretend to be a pediatrician. But I’m not hearing this description from them. I’m hearing some epidemiological pronouncements from them, which I disagree with.
But in terms of, but in terms of trying to characterize this disease, we’ve got to call it what it is.
Let me compare it to another mild disease. This other mild disease has a reproduction number of six or so, about the same as Delta. So it’s about as contagious as Delta and in most kids, it’s either asymptomatic or it’s the sniffles for a few days and then it goes away and then it clears up.
Let’s call that a mild disease.
The problem with calling it a mild disease is I’m describing polio. And that means that rarely, less than one percent—a vanishingly small proportion of kids—have serious neurological outcomes including severe paralysis in some cases.
It’s very rare. But I’ve never ever heard anyone call polio mild. If we refer to polio as a respiratory virus and invented something called long polio that we put in a different room for different people to talk about, we could call it mild.
So I think it’s very much: you’ve got to frame this virus for what it is, not for what we can see, not for what we would wish it to be. So long COVID, which is what happens after the respiratory phase, it’s still poorly defined. It’s difficult to study. The prevalence is anywhere from five to 40 percent, depending on how you use criteria in terms of the symptoms and the length of persistence of symptoms.
It’s very prevalent in children and, as I say, it’s very, very prevalent in children even if the children have a mild case—a mild, acute respiratory case. So it’s not a question if they didn’t look very sick, they didn’t get very sick. That’s not it.
It causes autoimmune disease that we call MIS-C, the inflammatory syndrome in children. And again, what I believe would be brain-tissue loss if we actually bothered to look.
Now, let me just say that Omicron is making the conversation even more complicated. Why? Omicron, appears to be, ironically, starting to behave like a respiratory virus.
And for adults, it seems to be that its ability to do the dreadful work—to do the systemic body work, to target the immune system, and to target the brain—that seems to be impaired in Omicron. And that’s really good news, sort of.
Because as it becomes a respiratory—or starts to behave more like a respiratory disease—it’s starting to hit children harder. And that’s what I’m really concerned about.
We have very little data about Omicron—and I don’t want to listen to anyone talk about severity of COVID in kids using old data. We’ve got to talk about Omicron data.
It’s absolutely pointless to look at what kids used to experience before Omicron. Omicron is what we need to be worried about and it’s different. It’s absolutely different.
We can show that first slide I have, which is U.S. hospitalizations.

We have done lousy data tracking in Canada. I didn’t want to use U.K. data because they count things differently. They count admissions differently. They’re mixing together ‘admitted because COVID’ versus ‘with COVID’. But the U.S. has excellent reporting. And this is typically the picture that makes people go ‘See, see, I told you so. It’s not very serious.’
But as an epidemiologist, I look at this graph and it honestly makes my blood run cold. It’s that orange-yellow line at the very bottom that looks so flat while all other age groups are rising and falling. That line just looks so flat except at the very right—if you see at that very bottom right corner just above the words Jan 2022, it starts to inflect up.
Now look at that. It’s way higher than at any point previously in the pandemic even though the overall population prevalence isn’t nearly what it was, let’s say, back in January 2021. So we’ve seen all of the sudden, childhood hospitalizations jump by a huge degree.
The only reason—there’s a mirage here—the only reason it looks low is because the y axis is scaled for very large numbers. If we simply took that off, and produced this graph—which, by the way, I can’t easily find out there—if we produced it just for this age group, we could use a scale that would make your blood run cold, too.
Hospitalization, child hospitalization, is way up with Omicron.
Yes, more mild for adults. Yes, more mild with respect, perhaps with respect, to long COVID—autoimmune disease, brain damage—but it’s putting way more kids in the hospital.
And we only have vanishingly recent data for this. And so it’s easy to dismiss, saying ‘Well, that could just be a bump.’ The problem is: it really isn’t a bump. It’s the beginning of what is, what looks like a pretty big incline.
So that’s a long, that’s a long way to look at, uhm a long answer to a short question.
I’m not quite done yet. If we could show the next slide.
Let’s sort of dig into ‘what does that little bend in that orange-yellow line really mean?’ Okay, so based on previous waves, we thought about one in 200 children with COVID were hospitalized. Estimates vary in different places but they kind of converge around there. And I accept that overall, hospitalizations with Omicron are actually a lot lower. Again, mild for adults.
So let’s assume for a moment that it’s milder for everyone. Instead of one in 200 kids to be hospitalized, we might expect one in 400 to be hospitalized, right? That’s what we might expect if kids were behaving the same way as adults with Omicron.
But if we look at just the last week of December in the U.S., they had 325,000 cases in the under-18 age group. This is across the entire U.S. So that’s a big number but it’s in a big population.
They had 4,700 hospital admissions per week. So that’s what that looked like.
That’s one in 70 being hospitalized.
Now, I want to be clear. That’s probably a big overestimate. Right? And the reason for that is the denominator.
We’re probably under-detecting COVID in kids for the reasons that we always have. We pay less attention. The cases aren’t as severe. And of course, now in the U.S. and elsewhere, we’re just unable to test. We’re unable to detect all the cases.
So there’s a different way to compare these. In other words, I want to be able to take this data from the U.S. and instead of just giving you an inflated number and be afraid, let’s look and see what this would be like if we mapped the U.S. numbers to B.C.’s population.
So, if you can go to the next slide, please.
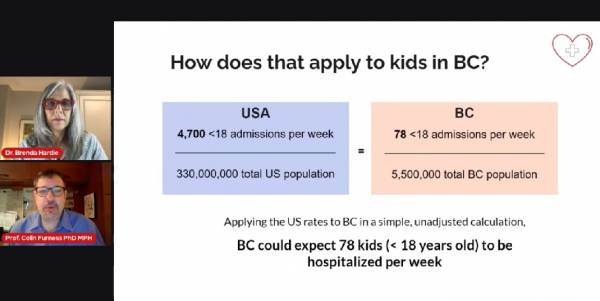
So if we said there were 4,700 admissions per week in the U.S., for the denominator, instead of trying to guess cases, let’s just use the overall population. It’s crude. It’s unadjusted. It’s a very back-of-the-envelope way to do this, but it’s actually quite clear.
That is to say that for a population of 330 million people, that produced 4,700. So we know the population of B.C. is much smaller. It’s about five and a half million.
So if we adjust that, we see that it turns out to reflect just about 78. If Omicron behaves in B.C. the same as it does in the U.S., we would expect about 78 admissions per week.
But here’s the problem, and I’m going to go to the next slide.

The problem is that that yellow-orange line is tilting upwards. It’s not a straight line. In other words, the rate of increase itself is increasing.
So hospitalizations in that last week of December in the U.S. increased by 65 percent over the prior week.
So let’s assume for a moment that orange line turns into a straight line. It turns into a diagonal straight line and it doesn’t arc up any further.
We could expect—week one, week two, week three, week four—we could expect this giant total of nearly 800. Nearly 800 admissions—child admissions—in B.C.
Now, that’s not necessarily critically ill. But not necessarily at all. But that is a very large number. This rate of increase may continue. It may pick up speed. It may level off.
The fact of the matter is truly, we don’t know. This is a very simplified projection, assuming that what we see in the last week in December in the U.S. that it applies to B.C. and continues in the same direction.
So it’s a very simple representation, but it is alarming. Because that is 800 child admissions to hospital within one month in B.C., I think would be—it would be really quite a strain.
So, that’s my way of saying: is it mild?
Well, if we had 800 mild admissions, we might just say ‘Okay, we’re going to have to put up with it. Maybe we’ll have some stretchers on the floor for a while.’
But we have to get back to that question now: what’s Omicron doing to kids? Let’s look at the next slide, please.
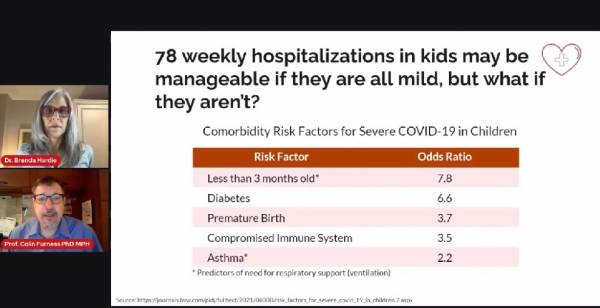
So, risk factors for serious COVID. Okay, so 78 weekly hospitalizations—maybe manageable if they’re mild.
But if they aren’t, let’s look at some of the risk factors for serious COVID, being less than three months old. That frightens me because the odds ratio is 7.8.
That means you’re 7.8 times, almost eight times, as likely to develop serious COVID requiring hospitalization if you’re under three months of age.
Now, we can’t stop people being under three months of age and we can’t isolate them from their parents and their siblings and the community.
We can’t Saran-wrap them. We can’t. So they are enormously at risk.
Diabetes, very prevalent in kids. Far more than it ought to be. That increases your odds of serious COVID by 6.6 times.
Premature birth, which has immune-system implications—3.7 times.
A compromised immune system, which a lot less kids have, it’s far less prevalent: three-and-a-half times.
And asthma, which is fairly prevalent in kids, more than doubles the chance.
Now, of these—being very young, under three months, and having asthma—those are significant predictors for requiring ventilation. And when kids need to be ventilated, you know that they’re seriously, seriously ill.
My understanding is that British Columbia has 27 acute-care beds [Furness later told the Straight that he meant to refer to pediatric intensive-care-unit beds and that he slightly misspoke] that it shares with the Yukon. That’s not very many [pediatric intensive-care-unit] beds if we have a bunch of kids under three months old and a bunch of kids with asthma becoming ill.
So that’s my answer to your question: is it’s mild?
Mild for some. Mild for adults. Milder than it was in those cases.
Yet child hospitalizations are going up and I’m worried. And I’ve got to say I’m not looking at Omicron as a mild ride for kids.
Dr. Brenda Hardie: Okay, thank you for that detailed answer. It helps us to get a little better picture.
I think quite a few folks have also been trying to get across this message that even if it is milder, a smaller percentage of a very large number can equal a very large number that will overwhelm our health-care system.
And if those happen to be pediatric patients in particular, B.C. is very vulnerable to overwhelm, given our very small number of pediatric ICU beds and also our geography—so many people living in remote and rural communities, infants being transported to our highly specialized centre in Vancouver.
This is just not a prospect that anybody really wants to have to think about. But this in fact may be what is coming.
A small shift but still sticking with a little bit of the basics of COVID and Omicron.
Why do you believe there is some debate about whether or not COVID is airborne? About the airborne transmission?
Colin Furness: I have a shorter answer. And this is a white-knuckled answer. We need to stop talking about whether it’s airborne.
In July 2020, 239 scientists wrote a letter to the World Health Organization and they said ‘Here is evidence that cannot be explained by droplet.’ That’s all they said. ‘It can’t be explained by droplet. We need to consider airborne.’
And there was a huge backlash. There was an enormous backlash that said ‘No, respiratory viruses are droplet. They’ve always been droplet. All of our evidence says that it’s droplet.’
We can have a long talk about scientific evidence and evidence quality, and how the evidence was understood. I want to leave that for a different time.
But just what I would like to say is that this, to me, this represents what some have called the Sasquatch problem. You only need one Sasquatch to prove Sasquatch.
So when you have transmission events that can’t be explained by droplet, you need to look for another explanation. And that’s something that a lot of people hadn’t wanted to listen to.
It was my colleague and former teacher David Fisman who made a very powerful point not long after. He said the reproduction number sounds low. It looks like it’s in line with respiratory diseases. But it’s an average.
Most people back in those early days of COVID didn’t give it to anybody. But once in a while, someone would give it to dozens of people. And that doesn’t happen with respiratory spread. It really doesn’t.
Or you can say ‘Well, it’s a wedding. Maybe one person hugged absolutely everyone, and that’s how it happened.’
But then you’ve got restaurants and buses and places where people aren’t actually hugging and interacting and moving around and you still have transmission. Not a lot of it. But again, how many Sasquatches do you need to be able to say Sasquatch is real.
And so the phenomenon, I’ve got to say it, the phenomenon of super-spreader events, which we’ve known about since that Washington choir way in early days of COVID, that tells us it’s airborne. It just does because we don’t see super-spreader events for things that only go short-range with droplets.
I looked at data for Toronto Transit Commission bus drivers. And what’s interesting about this is there was a belief that bus drivers might be at significant risk because they seemed to be getting sick a lot. So I compared the data from them with infection data from subway drivers and streetcar drivers.
Demographically, they are three similar groups so it’s a nice natural experiment. Well, bus drivers are the only ones that share with passengers. They’re surrounded by Plexiglas—just with little gaps on the side. You couldn’t sneeze on a TTC bus driver if you tried. But they’re still sharing air. Their rate of infection was a lot higher.
Again, smoking-gun evidence. Smoking-gun evidence.
That didn’t stop the Ontario government from going to court to argue against airborne spread. And I know that airborne has been resisted at the government and public-health level across the country at various times—particularly, particularly persistently in B.C.
We’ve got to stop talking about this. If there’s any doubt, the Omicron variant has now been estimated at its reproduction number to be at about 18.
That would make it right alongside the upper limit of what we think measles is. So it’s either as contagious as measles or more so.
Now, the thing about measles is someone with measles can leave the room and two hours later people walk into the room and get infected. Everybody gets infected. You can’t tell me that that is droplet.
By the way, measles is an RNA envelope virus. It presents like a ball with spikes. It’s morphologically very similar to COVID. It’s up in the air. It stays there.
Omicron is spreading with the same alacrity as measles. It can’t be droplet. It just can’t. And I think the final piece of it is more and more people are going to have absolutely no idea how they got infected.
It used to be almost two-thirds of people had no idea. Unless it was a family member, they really didn’t know. Now, it’s going to be almost impossible to find out where people got it from.
So, it’s airborne. Of course it’s airborne. And to deny that it’s airborne is simply to put people in harm’s way.
We have to stop talking about that. We can say ‘aerosol’. We can say ‘little droplets’. Whatever floats your boat. But we need to understand that it’s in the air and we have to stop talking about it.
More